

The Horrifying Truth of "Bottom Surgery" Part 1
The Real Risks and Outcomes of Vaginoplasties.

Part of the language that TRAs (trans rights activists) use is trying to glorify and sanctify these complicated surgical procedures. They will replace the surgical names with “bottom surgery” and they will often make the claim that these surgeries give trans people genitals that are indistinguishable from naturally developed genitals. This gives people a very dangerous misconception of what happens during these procedures.
The goal of this article is to educate people about the gruesome and graphic details of these procedures. This part will cover MtF procedures. There will be images of both surgical techniques and the finished results, both postoperative and fully healed. This is your only warning, if you are sensitive to these types of images, do not continue.
Vaginoplasty
A vaginoplasty for a trans person involves using the male anatomy to attempt to construct a “neovagina”. The “gold standard” for this procedure is called the penile inversion. This technique gives the “best possible outcomes” in terms of sensation and recovery. I will give the facts of the procedure and let you judge that for yourself.
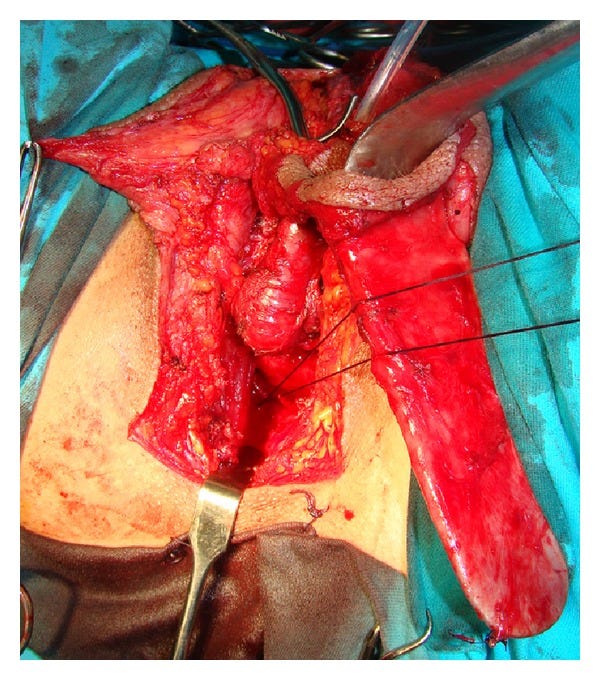
This “treatment” involves at least 1 prior surgery to remove the individual's testicles. For the beginning of this surgery, parts of the penis are marked so that a “clitoroplasty” can be formed. Next, the surgeons must dissect the penis into it's separate parts. This includes the removal of the corpora cavernosum, which must be removed all the way to the pubic bone. The corpora cavernosum is what causes the penile tissue to become erect. Once it is removed, the surgeons preserve the urethra, the penile skin, and the neurovascular bundle, which will carry sensation to the “neoclitoris.”

Once this has been done, the tube of what used to be the skin of the penis is inverted, as seen in the above image (left most tissue). The tip of that skin is then sewn to the ligaments of the sacrum, which if done incorrectly can result in nerve damage. In this image, they use an instrument to preserve the tube shape while they sew the “neovagina” in place.
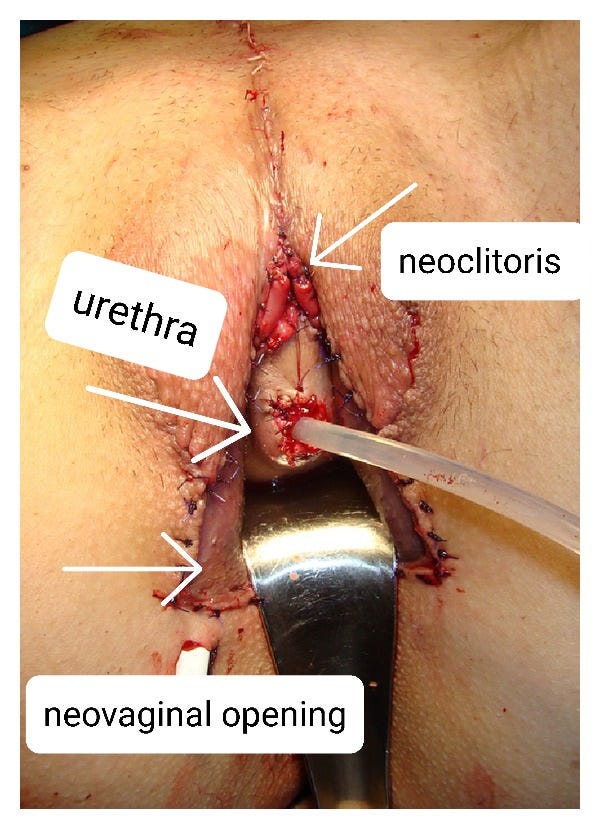
The urethra is then weaved into a pre-made urethral flap and sewn together. Once all of the pieces are sewn into place, the procedure is considered complete. The patient will have to remain on a urinary catheter for a while after surgery.
This was the outcome of this particular surgery.
There are various techniques that have been used to combat various complications in these types of procedures.
The first issue is the tendency for there to not be enough “depth” due to side effects of exogenous estrogen and puberty blockers, which can stunt the penile growth during puberty. To try and solve this issue, it is common to use a skin graft from either the inner thigh or from the scrotum. However, a common complication with using the scrotum is that it often results in hair growth within the neovagina. It is recommended that a laser hair removal procedure to remove the hair from the graft area prior to surgery, but recurrence of hair growth can happen. This results in “hair balls”…
The second issue is that the penile skin lacks the elasticity of vaginal tissue and lacks the ability to self lubricate. As an alternative, surgeons will use an intestinal or rectal graft as part of the vaginoplasty. While this certainly does allow for more elasticity, the lubrication produced by the rectum or intestines is very different from vaginal lubrication. If not properly sterilized, the intestinal tissue can also create a foul smell from within a neovagina. This is what has been reported by this poor soul.

Speaking of smells, part of female vaginal discharge includes a specific pH balance to help keep away the flora that can cause vaginal infections. Without this mechanism, the neovagina can be susceptible to bacterial infections.
In addition, complications that arise from neovaginas include fistulas. A fistula is when a tunnel forms connecting different organs. Fistulas that occur in neovaginas can include rectoneovaginal fistulas (tunnel between the rectum and the neovagina) and urethroneovaginal fistulas (between the urethra and the neovagina). This causes issue with infection from urine and feces getting into the neovagina.
Then there are complications that include things like graft necrosis, where the skin used starts to die. Other wound healing issues can occur between 4-16.8% of cases. This is an example of poor wound healing that requires “revision”.

More about these complications can be read about here: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8726601/
And for those of you who need examples of the finished product after it has healed, here are a few…



Finally, the discussion on sexual satisfaction of these neovaginas. The article that discusses the procedures says that following these surgeries, between 20-30% of patients were not able to achieve an orgasm.
Overall satisfaction is unclear as the patients in the study did not do long term follow-ups.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4058296/#!po=28.7234
So the next time someone mentions that a "transwoman” has had “bottom surgery”, this is what they are talking about.
Next time a child says they want “bottom surgery”, this is what they are talking about.
Next time a person argues “if a trans woman has had bottom surgery so they are female”, this is what they are talking about.
This surgery is considered “gender affirming care”.
I worry for the people that aren't getting the best care. Surgeons are notorious for making money off surgery and turning a blind eye to how much it helps/harms the patient. The culture of not talking about this is making it worse.
I think it's time for a reckoning.